
What do you do if a doctor isn’t around for miles?
What do you do if they’re just too swamped with other patients?
When your family needs medical care most in the case of a disaster, catastrophe, or emergency, what do you do?
In every thought experiment, every emergency scenario, the doctor is always going to be in high demand. In a catastrophe, there will only be so many people with medical training and a whole lot more people in need of medical care. Not only do you need the skills and overall understanding of how the human body functions, but you also need to have your checklists and medical inventory prepared and planned, ready to go in any emergency because injuries and life-threatening scenarios can happen in a split second. In disasters, supply chains get disrupted, toilet paper and baby formula randomly become scarce, and you will never know if the medicine for your health or the care of your loved one will be difficult to obtain.
For your homestead or camp, once you’ve made sure everyone in your family or group knows where the first aid kit is located, let’s take some time to review your basic-to-advanced medical emergency preparedness, skills, and checklists.
Medical Emergencies that Require Immediate Attention
- Heart attack OR cardiac arrest– the heart stops working correctly due to heart disease in one, randomly in the other. Cardiac arrest is a bioelectrical problem; a heart attack is a circulation issue.
- Stroke – a blood vessel in the brain weakens to the point of perforation or bursting, spilling blood in the brain where it isn’t supposed to be.
- Head or spine injury – any injury to your body’s main conduit of electrical signals
- Bleeding – of varying degrees, from surface level to arterial/venal (arteries and veins)
- 2nd & 3rd-degree burns – (2nd) blisters and some thickening of the skin (the most common severe burn) (3rd): widespread thickness with a white, leathery appearance, definite nerve damage.
- Chemical and electrical burns
- Breathing difficulties: stopped breathing, blocked breathing passages, changes in breathing patterns, shortness of breath, hyperventilation, or choking
- Fainting, collapsing, blacking out, sudden loss of memory
- Seizures of varying types
- Severe, unexplainable pain
- Eye trauma or change in vision
- Shock
- Unusual behavior, confusion, difficulty wakening
- Sudden dizziness, weakness, or fatigue
- Coughing up or vomiting blood
- Smoke inhalation
- Near-drowning
- Ingesting or being exposed to a poisonous substance
- Severe abdominal pain or pressure
- Broken bones (there are at least 9 other types of breaks beyond compound fractures, where bone protrudes from the skin), depending on how the bone’s been broken
For a breakdown of how to deal with the full list of the above emergencies, jump to the end for the medical supply checklists, extended links, and extensive field manuals from the U.S. Military.
What to do: Head & Spine Injuries
- Keep the person still. Place heavy towels or rolled sheets on both sides of the neck or hold the head and neck to prevent movement.
- Avoid moving the head or neck. Provide as much first aid as possible without moving the person’s head or neck. If the person shows no signs of circulation (breathing, coughing, or movement), begin CPR, but do not tilt the head back to open the airway. Use your fingers to gently grasp the jaw and lift it forward. If the person has no pulse, begin chest compressions.
- Don’t roll alone. If you must roll the person because he or she is vomiting, choking on blood or because you have to make sure the person is still breathing, you need at least one other person. With one of you at the head and another along the side of the injured person, work together to keep the person’s head, neck, and back aligned while rolling the person onto one side.
Heart Attacks Vs Cardiac Arrest – Emergency Responses Differ

When To Use CPR
CPR should be performed on a person if they are unresponsive and not breathing normally.
Someone may be unconscious, unresponsive, and not breathing normally due to:
- Accidents
- Near-drowning
- Suffocation
- Poisoning
- Heart attacks
- Drug overdoses
- Smoke inhalation
- Electrocution injuries
- Suspected sudden infant death syndrome (SIDS)
How to Do CPR
First, examine the scene for any obvious hazards. In some cases, it may not be safe to perform CPR. If there are any dangers nearby preventing you from getting close to the person, don’t endanger your own life as well as theirs. Call emergency services and wait for help to arrive. If emergency services are not up and running, move forward to the next step, but while keeping the following two bullet points in mind:
- For example, if the person has collapsed due to exposure to smoke and fire or toxic fumes, steer clear of the area.
- If the person is in a dangerous situation and you’re able to move them safely, do so before trying to give them CPR. For example, if they’ve collapsed in the middle of the street, wait for a moment when there’s no oncoming traffic and then move them out of the road.
Second, check for unresponsiveness. If an adult or teen collapses but remains conscious, CPR is not typically needed. If they lose consciousness and are not breathing, however, you should administer rescue breaths if possible, or stick to hands-only CPR if you’re not trained in doing rescue breathing. If they’re not breathing, have no pulse, and are unresponsive, try to perform some form of CPR even if you are untrained or rusty in your abilities.

- Shake the victim’s shoulders and loudly ask, “Are you okay?” If you receive no response, check for signs of breathing, like the person’s chest rising and falling. Check for a pulse by placing your fingers on their carotid artery, next to the windpipe just below the jaw.
- Hands-only CPR is ideal for those without formal CPR training or for people unsure of their CPR abilities. It does not involve the rescue breathing measures associated with conventional CPR but instead focuses on chest compressions
Third, call for help if you can. After checking the scene and the victim’s responsiveness, this is the time to ask for help and/or call emergency services. If you find a person who is unresponsive, isn’t breathing, or doesn’t have a pulse and you decide to do some form of CPR, you should still immediately call for help before you do anything else. CPR can revive people on occasion, but it should be viewed as buying time until emergency personnel (or someone more experienced in emergency medicine) arrives with appropriate equipment in every training and emergency scenario.

- If 2 or more people are available, 1 person should call for help while the other begins CPR.
- If a person is unresponsive because of suffocation (from drowning, for example), then it’s recommended to immediately begin CPR for 1 minute and then call for help again.
- If the victim is a child between the ages of 1 to 8 years, perform 5 cycles of chest compressions and rescue breathing before calling for help if you are the only person available. This should take roughly 2 minutes.
- Calling official emergency services will bring paramedics to the location. Typically, the dispatcher (the personnel on the phone) will also be able to instruct you on how to perform CPR.
Fourth, keep the victim on their back. In order to perform hands-only CPR, the victim should be positioned in a supine position on their back, preferably on a firm surface, with the head facing up. If the person is on their side or stomach, then gently roll them onto their back while trying to support their head and neck. Try to make note if the person experienced significant trauma while falling and becoming unconscious.

- Once the person is on their back, kneel next to their neck and shoulders so you have better access to their chest and mouth.
- Keep in mind that you should not move the person if you suspect they may have suffered a significant head, neck, or spinal injury. In this case, moving them is life-threatening and should be avoided, unless emergency help won’t be available for a long time (a few hours or more).
Fifth, tilt the person’s chin up to open their airway. Once you have them on their back, tilt their head back while pressing their chin up and forward with two fingers. This should move their tongue out of the way and make it easier for them to breathe.
- If you’re afraid the person has a neck injury, try not to move their head. Use both hands to carefully move their jaw forward without moving the rest of their head or neck.
- Once you’ve opened the airway, listen carefully for sounds of breathing and check to see if their chest is rising and falling. If the temperature outside is cold, you can check for misted breath as well. If you can’t find any signs of breathing after about 10 seconds, or if the person is only gasping occasionally instead of breathing regularly, start CPR.
Sixth, rhythmically push down on the center of the chest. Place one hand directly over the center of the person’s chest (between their nipples, generally) and your other hand on top of the first for reinforcement. Press down on the victim’s chest firmly and quickly—aim for about 100 chest compressions a minute until paramedics arrive.

- If you’re not sure what 100 compressions a minute really means, try doing your compressions to the beat of the Bee Gee’s song “Stayin’ Alive”, or Queen’s song ‘” Another One Bites the Dust”.
- Use your upper body weight and strength, not just your arm strength, to push straight down on the chest.
- Your chest compressions should cause the person’s chest to depress at least 2 inches (5.1 cm). Push hard and understand that it is likely you will break the person’s ribs. This is extremely common, and you shouldn’t stop compressions even if you think this has happened.
- Chest compressions are hard work and you may have to switch off with other bystanders before emergency personnel arrives. If there is no emergency personnel, continue rotations.
- Continue doing this action until the person becomes responsive or until the emergency medical team arrives and takes over.
When to Treat Burns as an Emergency
A burn can result from any source of excess heat that damages body tissue. Burns can be minor or life-threatening, which is why knowing first aid treatment for burns is essential. Prompt attention can limit damage and promote healing. It’s serious when:
- Blisters are larger than 2 inches
- Blisters are on the face, hands, or genitals.
- Pain lasts for more than a few hours
- Looks white or charred

How to Treat Second-Degree Burns
A second-degree burn causes redness, blistering, pain, and swelling.
First, immerse the area in cool water for at least 10 minutes. Do not use cold water or ice. It may take as long as half an hour for the pain to go down.
Second, remove jewelry or clothing that could become too tight if the area swells.
Third, do not put grease, butter, ointment, or powder on the burn.
Fifth, if you are treating the burn at home, wash your hands and gently rinse the burn, then dry it with a clean, soft cloth.
Sixth, never break a blister, as it increases the risk of infection. They will break themselves in about a week.
Seventh, if blisters are intact, you do not have to bandage the burn. If they have broken open, wrap the burn loosely in a nonstick bandage, preferably one made for burns.
Eighth, change the dressing anytime it gets soiled.
Last, if the burn is larger than 2–3 inches, or on the face, hands, genitals, or a major joint, see a medical provider promptly or understand that it’s quite serious.
Can I Treat Third-Degree Burns?
Third-degree burns, which reach the layers of fat and other structures under the skin, can be life-threatening. Treatment of third-degree burns in the field or in an emergency setting is extremely difficult. Third-degree and fourth-degree burns may need more intensive treatments such as intravenous (IV) antibiotics to prevent infection or IV fluids to replace fluids lost when the skin was burned. They may also need skin grafting or the use of synthetic skin.
- Do not soak the burn with water.
- Do not apply any ointment, butter, grease, or spray.
- Do not remove clothing that is stuck to the area.
- Cover the area with a sterile bandage or a clean loose cloth.
- Remember, third-degree burns may not be painful if the nerve endings have been damaged. Even if there is no pain, prompt medical care for a severe burn is essential.
Chemical Burns
A chemical burn may be felt immediately or it may take time to develop, depending on the cause. If the burn is deep or bigger than 3 inches, call 911 or again, understand that you’re in a critical situation. If you have it, bring the container with the chemical with you to the ER.
Take the following first aid measures for a chemical burn:
- Wear protective gloves and brush off any dry chemicals.
- Then flush the area with cool water for at least 10 minutes.
- Remove any clothing or jewelry that may have touched the chemical.
- Cover the area loosely with gauze or a nonstick material or cloth.
- If the area begins to hurt again, repeat flushing with cool water.
Electrical Burns
Immediate medical assistance for electrical burns is essential. Electrical burns can be worse than they look on the surface. If you have an electrical burn from lightning, electrical wires, or household objects, see a healthcare provider promptly. If you are assisting someone, do not touch them if they are still in contact with the source of the electrical shock or burn.
Having been electrically burned, the following symptoms are experienced:
- Severe burns
- Confusion or loss of consciousness
- Difficulty breathing
- Muscle spasms or seizures
When it is safe for you to touch the person, administer CPR if you are trained and the person is not moving or breathing.
Try to keep them warm and drape a clean cloth over the affected area.
Do not use materials with fibers that may become stuck to the wound.
When to Stop Bleeding
Major bleeding can cause someone to lose consciousness or die within minutes. That’s why tourniquets are kept on the outside of gear bags for rapid access.
Most people tested in laboratories stop bleeding from one minute to nine minutes. (mountsinai.org, 2022) When a wound, cut, or an injury produces bleeding, well-aimed direct pressure is the definitive way to stop bleeding. Serious hemorrhaging can cause someone to bleed out in under a minute; when you see blood, your first priority is to slow down and mitigate blood loss.
- Wear gloves and a face shield whenever possible
- Elevating the wound above the heart is helpful because it reduces blood pressure to the injury
- The most common error is not holding pressure long enough — hold firm for at least 5-10 minutes
- Resist the urge to peek at the wound, otherwise, you might lose your progress
- Don’t let patient discomfort prevent you from doing what you need to do to help them
Your Basic Guide to Stopping Bleeding in Bullet Points (if you have super limited time in an Emergency)
Move down to each bullet point if the bleeding just doesn’t stop:
- Elevate the bleed above the heart.
- If that doesn’t stop it, put pressure on the wound.
- If that still doesn’t slow down the bleeding, it’s a tourniquet time.
How to Stop Bleeding
First, put on your gloves or sanitize. if it’s wet and not yours, don’t touch it bare-handed. A bloody injury is a good example of when you should pause to be thoughtful and careful. In all but the most severe every-second-matters injuries, it’s worth taking a moment to protect yourself by putting on protective gear before exposure to other people’s fluids.

Second, elevate the wound above the heart, aiding with the natural clotting process.
“You make it easier and faster for the body to build that dam when it doesn’t have a flood of blood constantly screwing up the construction site.”
https://theprepared.com/survival-skills/guides/stop-bleeding/
Third, remove any clothing or debris on the wound. Don’t remove large or deeply embedded objects. Don’t probe the wound or attempt to clean it yet. Your first job is to stop the bleeding.
Fourth, stop the bleeding. Place a sterile bandage or clean cloth on the wound. Press the bandage firmly with your palm to control bleeding. Apply constant pressure until the bleeding stops. Maintain pressure by binding the wound with a thick bandage or a piece of clean cloth. Don’t put direct pressure on an eye injury or embedded object. Secure the bandage with adhesive tape or continue to maintain pressure with your hands. If possible, raise an injured limb above the level of the heart.
Even in advanced situations where you’re using an absorbent material to pack a deep or hard-to-reach wound, the whole point is to create pressure when your fingers alone can’t do the job. You don’t pack a wound simply to absorb blood while waiting for the clot to form.
In 2010, the American Heart Association claimed that limb elevation was not an effective way to stop bleeding and may even be harmful. The AHA argued that there weren’t enough studies proving the effectiveness of elevation — but there weren’t any disproving it, either. They’ve since retracted because recent studies have proven that elevation is appropriate and useful.
How to use a pressure dressing
Consider a pressure dressing for simple wounds on the extremities, torso, or head. Pressure dressings are sometimes called “Israeli” dressings. Pressure dressings are an absorptive material combined with an elastic bandage and rigid “pressure bar” that makes it easier to focus pressure directly over the bleeding source – a combo between plain dressings and a tourniquet.
Tip: Don’t pull too tightly — the point isn’t to cut off blood flow to the whole area the way a tourniquet would. Check the patient’s fingers or toes afterward for proper circulation.
Tip: You can improvise an OLAES-style pressure dressing using gauze, an elastic bandage, and a small rock. Place the dressing against the wound like normal. Begin wrapping the elastic bandage. Part way through the wrap, place the rock directly over the wound. Finish the wrap, wedging the rock in between layers of the somewhat tight bandaging.
When to pack a wound
There are places on the body — such as the armpit, groin, and neck junctions — that are just too difficult to create well-aimed direct pressure against. Or sometimes a wound is so deep that you can’t push hard enough on the surface to create pressure down at the point of severe hemorrhage.
Packing a wound is the process of building pressure by forcing gauze (or similar material) into the wound.
How to pack a wound
First, if it’s a serious bleed, stick your finger or thumb into the wound. Try to find the source of bleeding and push against it without making the wound worse.
Second, take the gauze out of its packaging. Start rolling one end of the gauze into a tight ball (sometimes called a speedball). That ball will be the first thing you push into the wound, so it should be a little smaller than the size of the wound but have enough heft to make the pushing easier.
- Tip: If the gauze is rolled, you can poke the tightly-wound middle of the roll out with your fingers and use that as your starting point.
Third, push the gauze ball into the wound channel alongside the finger you already have inside.
Fourth, relax your finger just enough to swap places with the ball, immediately pushing the ball as deep and forcefully as needed. Create another wad in the gauze near the wound entrance. Stuff it down. Repeat.
- If you have enough material, eventually you’ll build the pack up until it reaches the surface. It’s then much easier to use your fingers to press down on the pack, transferring that pressure down onto the blood source for 10 minutes.
What about internal bleeding?
The short answer: If someone has internal bleeding in a bad survival scenario (no professional help, no grid, etc.), they’re probably going to die.
You just can’t create enough well-aimed direct pressure inside the belly without opening up the patient. Some studies have also shown that trying to create enough pressure on an organ from outside the body can further tear the wound and accelerate blood loss.
The exception would be when the internal bleeding isn’t so … internal. If someone has been torn open in such a way that you can get access to the source, then it might be worth applying pressure if all other hope seems lost.
theprepared.com/survival-skills/guides/stop-bleeding
Should you use tampons for hemorrhage control?
Using a tampon to plug an injury (e.g. a bullet wound) is such an incorrect-but-still-popular “prepper hack” that it made our list of the worst survival myths.
Tampons are designed to absorb blood. They do that job well. You can even split tampons open and use them as extra gauze (or even fire-starting tinder) if you run out of proper materials.
Tampons and menstrual pads do not expand enough when soaked to apply pressure to a wound. Since bleeding is controlled through direct pressure, even in a bullet hole, a tampon is no more effective than simply putting in a few loose layers of gauze.
If you plug a bullet hole with a tampon, all you’re doing is creating an absorbent dam in the first few inches near the surface. Like a dam on a river, that will create a reservoir pool of blood. That’s not necessarily bad — but it’s definitely not helpful.
theprepared.com/survival-skills/guides/stop-bleeding
When to Dress a Wound
It’s worth noting that open wounds are a doorway for germs and, subsequently, illness – which can result in worse problems. Even a minor cut might need cleaning and sealing shut. Wound dressings are used to protect yourself and injury from the external environment. They can be used to clean, cover, and protect you from the elements and infection.
- A wound dressing must provide a moist environment, remove the excess exudate, avoid maceration, protect the wound from infection and maintain an adequate exchange of gases (the wound needs to be able to “breathe”).
How to Dress a Wound
First, wash your hands. Before dressing the patient’s wound, wash your own hands with a gentle soap. If you have gloves handy, put them on.
Second, press using a clean washcloth or clean 4×4 gauze pads, and apply pressure to the wound until the bleeding subsides. If the bleeding does not discontinue after five minutes, you should seek additional medical attention.
Third, clean the wound first (and daily afterward) with mild soap and water. Choose a soap that does not contain any fragrance, dye, or antibacterial ingredients. You may choose to put hydrogen peroxide on the wound, but it can burn and isn’t entirely necessary. Never use alcohol, as that will create an intense burning sensation.
Fourth, pat the area dry with a clean towel or gauze pads. Be careful not to rub or wipe, but gently dab the area.
Fifth, dress the wound. Depending on the nature of the wound, you can choose to cover it until a scab forms or leave it open. If you decide to cover it, use a bandage or gauze and medical tape, being careful not to put any adhesive on the wound. Avoid touching the cloth part of the bandage so you don’t contaminate it. Don’t enclose the bandage on all four sides.
The body has an innate ability to heal through scab formation, so allowing that process to take place is good. Avoid swimming or sitting in the bathtub, which can cause the scab to come off. Also, avoid picking at the scab, as this can disrupt the healing process and cause infection.
Last, what to watch for: if you notice any signs or symptoms of infection, call your physician or someone more experienced immediately.
These symptoms include:
- Intense redness around the wound site,
- Hot to the touch,
- Discolored or foul-smelling drainage,
- Any type of fever or sharp increase in pain.
If the cut involved any metal or rusty objects, make your physician aware, as the patient may need a *tetanus shot.
What is the first aid for tetanus?
A thin layer of an antibiotic cream or ointment to discourage bacterial growth and infection. Doh.
Note: Bandage reasonably. Tourniquets should only be employed as a last resort. And that’s because a limb’s tight-binding might induce its loss. So, unless it’s a matter of life or death, using a tourniquet isn’t something to think about.
Although it is vital that you clean the wound and dress it with a clean cloth, if one is accessible, you should be sure to close any new wounds with a sterile cloth. Change your bandages on a regular basis because a filthy bandage might lead to an infestation.
When to Use a Butterfly Bandage for First Aid
A butterfly bandage may be used to close a minor cut that is deep but not wide. It should be utilized on a straight, not jagged wound. A gaping wound of that sort might remain open. To promote healing and minimize scarring, a butterfly bandage can be used to seal the injury. A butterfly bandage is most effective on a wound that measures less than two inches in length. More than one bandage can be used to close a cut that is longer than two inches.
How To Use A Butterfly Bandage for First Aid
First, stop the blood flow. Stop the blood flow by applying pressure, preferably with a clean compression pad/gauze, when treating any wound.

Second, clean and disinfect the wound. Use clean water to flush any debris out of the wound.

Third, apply the bandage across the width of the cut. Start on one side and wrap the bandage around the wound. After that, press the skin together to close up the cut, then apply the other side of the butterfly bandage to the skin on the opposite side.

Fourth, apply additional bandages. The first butterfly bandage should be centered over the wound. Some people like to apply extra bandages even if the injury is minor. They approach this one from angles, making an X over the initial bandage. This technique allows for greater skin capture, which helps hold the wound in place better.
Fifth, apply antibiotic. You want to apply topical antibiotic ointment on areas of the wound that have not yet healed and different parts of your body. You’ll need to reapply the antibiotic ointment once or twice a day.
Sixth, cover the wound with gauze and adhesive. To keep the bandage in place and the wound clean, cover it with gauze and tape. If you use a butterfly bandage to wrap a cut, maintain the bandage until it peels off on its own. It might take 10 to 14 days for the wound to heal.
When to Suture and Stitch
Sutures are used when a wound is deep and interior tissue is visible. If you can see fat or subdermal layers in the wound, start prepping your needle via sterilization, and your monofilament sutures (one single thread). If you just tried to close the wound with a bandage, it would only bring the top part of the tissue together, leaving the tissue beneath still separated. Healing and recovery on a cellular level (the clotting process with platelets) speed up when similar tissue is “bonded” together. As long as your wound was sterile, you’re well-versed in treating infections with multi-threaded sutures, you’ll heal well and with minimal loss of function.
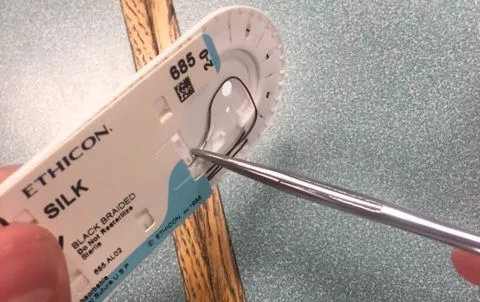
How to Suture & Stitch (with Pictures)
Gather the necessary equipment:

- A suture pad, [or real flesh in the emergency]
- Tissue forceps: opens up the wound and allows clear vision of the needle’s puncture site
- Scissors: To cut the excess thread.
- Needle holder: To prevent the spread of germs, the needle must always be held by the needle holder rather than being held with your hands.
- Needle with thread: The choice of the needle size and thread type depends on the reason for performing a suture and the nature of the wound. The needle with thread used in the following steps is 2-0 silk.


How to Instrumental Tie








First, using the tissue forceps, expose the skin towards the end of the right side of the wound. This allows for better visualization and avoids hitting muscles.
- This step should always be done before puncturing the skin, which is introduced in the next step.
- Remember to always avoid pushing down on the skin with the tissue forceps.
Second, puncture the right side of the skin (take a bite). Aim for about half a cm down from the end of the wound with a 90 degrees angle between the skin and the needle, twisting your hand clockwise for about half a circle.
- The needle goes through the skin from outside to inside.
- Also, make sure that the needle exits on the inner side of the skin; it should go down to a depth of about 0.5cm.
- To release the needle holder’s “click” to pull the needle out, pull the needle holder with your ring finger to the right and push with your thumb to the left.
Third, parallel to the first bite, puncture the left side of the skin the same way as you did in the last step. However, in this step, the needle goes from inside to outside.
Fourth, hold the needle with the needle holder (without the need to hear a click) and pull so that all the thread, except for about 3–5 centimeters (1–2 in), is on the left side of the wound.
Fifth, after releasing the needle from the needle holder, use your left hand to hold the thread near the wound and wrap it approximately a cm or two from the tip around the closed needle holder.[5]
- Make sure to wrap the thread three times outward (clockwise) while keeping the thread in close proximity to the wound.
- Note: The direction in which you wrap the thread does not matter as long as it alternates between consecutive steps.
Sixth, slightly open the needle holder with the thread wrapped around it, and grab the 3–5 centimeter (1.2–2.0 in) of thread on the right side with the needle holder.
Seventh, using your left hand, pull the long thread to allow the wrapped thread to pass out of the needle holder and get tied around the loose 3–5 centimeter (1.2–2.0 in) of thread on the right.
- Be careful to NOT pull too much on the skin, causing one side to be pushed on top of the other.
- Only pull as much as you need in order to bring together and seal the two sides of the wound.
Last, do steps 5 to 7 again with a couple of alterations:
- Note: these three steps (5 to 7) will be done a total of 3 times, with a small difference in them each time.
- First, do steps 5 to 7, wrapping the thread inwards (counterclockwise) twice around the needle holder.
- Then, do steps 5 to 7 a third time, wrapping the thread only once outwards (clockwise) on the needle holder.
When To Use a Tourniquet
When applying pressure alone to the wound doesn’t stop the bleeding. An artery or vein has been severely damaged and blood flow needs to be stopped to prevent bleeding out.
- Mass casualty events
- Vehicle collisions and accidents
- Falls
- Hiking accidents
- Knife wounds
- Shootings
How to Use a Tourniquet
Tourniquets are ONLY applied on limbs! Never on a neck!
Major bleeding control practices in areas not accessible by tourniquets (like the stomach and back) will be covered further at another time.
With that out of the way, here are the steps of applying a tourniquet:
First, wrap the limb with a rope/belt/bra at least two inches closer to the body than the wound. Do not apply a tourniquet over the joints – blood passageways are protected in joints, and you’ll never put pressure on the arteries. Therefore, the tourniquet won’t decrease bleeding.

Second, place it closer to the body than the joint. Then tie the tourniquet in place once using an overhand knot.

Third, place your desired torsion device (the long black piece in the image below) on top of the overhand knot. Tie another overhand knot, then another to secure the torsion device onto the tourniquet.

Fourth, twist the torsion device in one direction until the bleeding stops.

Fifth, secure the tourniquet in place. This can often be accomplished by using the loose ends from your last knot to tie one end of the torsion device to the tightened tourniquet, or to the limb. Write the exact time the tourniquet has been applied.

Removal of Tourniquets
Remember, a tourniquet is a two-hour solution. After that, one runs the risk of other complications such as infection, and loss of limb or life. You should never remove a tourniquet unless you know exactly what you’re going to do next. Refer to the field manual resources below and external links for what to do in the case a doctor is not around to remove the tourniquet. Think of it this way: once you apply the tourniquet’s torsion device, a 120-minute timer starts.
Types Of Tourniquets
In today’s military, all soldiers are issued tourniquets to accompany their armor and weapons, and every soldier is trained and proficient at applying his tourniquet–even one-handed on his own arm.
The best tourniquet is probably the one used by the army, the Combat Action Tourniquet (CAT tourniquet). Another great type of tourniquet is the Recon Medical.
If you don’t want to buy a tourniquet, luckily for you, tourniquets are everywhere.
Are you wearing a belt? Tourniquet!
Have laces on your shoes? Tourniquet!
Long sleeve shirt, bicycle inner tube, backpack strap, or a female brassiere? All tourniquets!
How To Make A Tourniquet
- Choose a wide, strong piece of material. A triangle bandage, scarf, or bandana will work. Avoid thin items such as phone cables if you can. Belts also will not work.
- Cross the material above the wound.
- Put a tightening rod in place. A stick or carabiner will work. Avoid items like pencils which can easily break.
- Make a knot around the rod with the tourniquet material.
- Twist the rod. You will need to twist tightly to stop blood flow.
- Secure the rod in place. This can be done by tying another piece of material around it. Hair bands will also work.
When to Splint
A splint is used when bones get broken, first used instead of casts due to extensive swelling common with bone fractures. Once applied, a splint provides temporary support and protection to the injured area as your body begins the initial responses to internal injuries and healing. Splints will increase the chances your bones are set well, straight, and aligned, not crooked.
How to Splint
First, check the CSM (Color, Sensation, and Movement) of an injured person before and after splinting. When dealing with emergency injuries, such as a broken leg, you can prevent complications by checking for “CSM” before splinting and regularly afterward until you get the injured person to a hospital. Watch for changes that happen after the splint is applied – that’s one way to know the splint is too tight or is otherwise causing problems. Checking the CSM before splinting gives you a baseline, and information to tell emergency services.

Color: Watch for reddening or paling of the injured extremity. If fingers or toes turn white, it means blood flow is restricted. Loosen or remove splinting right away to prevent serious complications.
Sensation: Check the injured person’s ability to feel sensations to make sure they’re not having nerve problems. Have them close their eyes or look away, and touch each toe or finger of the affected limb. Use firm pressure with your thumb and ask them to tell you when you’re touching them. Then check for sharp sensation by applying pressure to each digit with a pin or sharp stick.
Movement: A splint should immobilize a limb, but not prevent movement entirely. If the person loses ability to move a limb once a splint is applied, it could mean that swelling is causing the splint and wrap to be too tight. Remove the splint quickly.
2. Get creative to find supplies [or, just your splint you packed in your first aid kit]. You can splint a limb with any strong, straight object you can find. Find a stick, plank, or small log, or roll up a newspaper or towel to use as a splint. Shoelaces, ropes, belts, strips of clothing, or even vines can be used to hold the splint in place. Use excess clothing for padding.

3. Move the injured limb as little as possible. Moving an injured limb can cause further damage. Move the limb as little – and as gently – as possible to get it into a position in which you can splint it. Preferably, do not move it at all and apply the splint the best you can in the limb’s current position.

4. Place the splint to minimize movement of the injured area. In an emergency, you do not have to know the exact right way to splint an injured joint. Try to minimize movement of the affected joint or limb. The best way to do this is to apply a splint to the joint both above and below the injury. For instance, if the forearm is injured, apply a splint that extends from above the elbow to below the wrist. Secure the splint just below the wrist and above the elbow for best support.

5. Pad the area between the injured limb and the splint. Use something for padding such as clothes. Gently wrap the injured area in padding, but do not pull the wrap too tight. Provide cushioning between the person’s skin and the splint without interfering with blood circulation.

6. Apply the splint to one side of the injury. Use your rigid object to brace the injured limb. If there is an open wound or if bone is protruding from the skin, put the splint on the uninjured side of the limb, if possible.
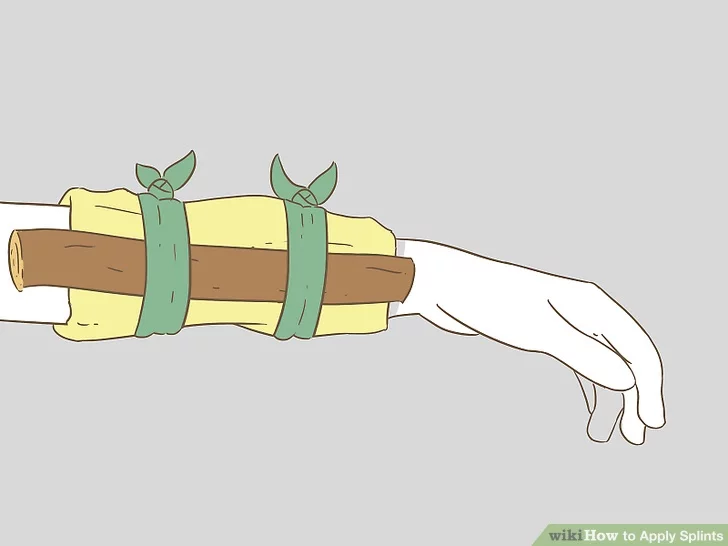
7. Tie the splint to keep it in place. Tie or tape the splint in place on both ends of the splint. Brace the splint on the outsides of the two joints surrounding the injury. This provides the best support. For instance, tie the splint below the ankle and above the knee for leg injuries.

If using tape, try to tape over the padding and not directly on the person’s skin.
Try not to tie or tape something directly over the injury.
If the elbow or shoulder is injured, tuck the arm close to the body and wrap the whole torso, immobilizing the limb against the body.
If one leg is severely injured and you will be able to carry the victim, splint the injured leg to the uninjured leg.
8. Use a SAM splint, if available. A good outdoor first-aid kit can include a SAM splint, a moldable aluminum strip between two layers of padding that hardens once put into position.

They are small, inexpensive, and lightweight, and can be a good temporizing measure in an emergency; though they do not provide much support. If using a SAM splint, follow these general guidelines:
Mold the splint on someone of similar size and shape to the injured person, not directly on the injured person. Once the splint is shaped, apply it to the injured person and hold it in place with anything you have: a sock, torn shirt, tape, cling film, or elastic bandages.
Do not wrap the splint too tightly; it should be snug, but allow room for swelling.
If you’re using anything from nature that can splinter, wrap it in clothing first.
When to Treat Shock
Shock is an emergency condition brought on by a sudden drop in blood flow throughout the body. Shock might result from trauma, heatstroke, blood loss, an allergic reaction, severe infection, poisoning, severe burns, or other causes. When a person is in shock, his or her organs aren’t getting enough blood or oxygen. If untreated, this can lead to permanent organ damage or even death.
Signs and symptoms of shock vary depending on circumstances and may include:
- Cool, clammy skin
- Pale or ashen skin
- Bluish tinge to lips or fingernails (or gray in the case of dark complexions)
- Rapid pulse
- Rapid breathing
- Nausea or vomiting
- Enlarged pupils
- Weakness or fatigue
- Dizziness or fainting
- Changes in mental status or behavior, such as anxiousness or agitation
How to Treat Shock
First, lay the person down, if possible.
- Elevate the person’s feet about 12 inches unless the head, neck, or back is injured or you suspect broken hip or leg bones.
- Do not raise the person’s head.
- Turn the person on the side if they are vomiting or bleeding from the mouth.
Second, begin CPR, if necessary.
If the person is not breathing or breathing seems dangerously weak:
- For a child, start CPR for children.
- For an adult, start adult CPR.
- Continue CPR until help arrives or the person wakes up.
Third, treat obvious injuries.
Fourth, keep the person warm and comfortable.
- Loosen restrictive clothing.
- Cover with a coat or blanket.
- Keep the person still. Do not move the person unless there is danger.
- Reassure the person.
- Do not give anything to eat or drink.
Fifth, follow up by checking blood pressure and other vitals.
When to Treat Poisoning
Symptoms associated with serious poisoning include:
- being sick
- dizziness
- sudden, noticeable heartbeats (palpitations)
- breathing difficulties
- uncontrollable restlessness or agitation
- seizures (fits)
- drowsiness or loss of consciousness
How to Treat Poisoning
If they’ve been poisoned by swallowing something, try to get them to spit out anything that is remaining in their mouth. If they’re unconscious, try to wake them and encourage them to spit out anything left in their mouth. Do not put your hand into their mouth and do not try to make them sick.
If a harmful substance has splashed onto their skin or clothes, remove any contaminated items and wash the affected area thoroughly with warm or cool water. Be careful not to contaminate yourself in the process.
While you’re waiting for medical help to arrive, lie the person on their side with a cushion behind their back and their upper leg pulled slightly forward, so they do not fall on their face or roll backward.

Wipe any vomit away from their mouth and keep their head pointing down, to allow any vomit to escape without them breathing it in or swallowing it. Do not give them anything to eat or drink.
If the person is not breathing or their heart has stopped, begin CPR.
Because there are so many factors to poison, with limited knowledge, it’s not prudent to try and specifically treat a poison you have little knowledge of. In this type of emergency, you’re very reliant on labs and experts to identify the best way to treat the toxins from poisoning.
Possible treatments that can be used to treat poisoning include:
- activated charcoal – sometimes used to treat someone who’s been poisoned; the charcoal binds to the poison and stops it from being further absorbed into the blood
- antidotes – these are substances that either prevent the poison from working or reverse its effects
- sedatives – may be given if the person is agitated
- a ventilator (breathing machine) – may be used if the person stops breathing
- anti-epileptic medicine – may be used if the person has seizures (fits)
When to Use the Heimlich Maneuver
When someone’s choking: food or other obstruction blocks airways and the person cannot breathe.
How to Do the Heimlich Maneuver
First, determine if the person is truly choking.

A choking victim will often have their hands around their throat. If you notice someone making this gesture, look for the following indications a person is choking:
- Cannot breathe or experience loud, difficult breathing
- Cannot speak
- Inability to cough effectively
- Blue or gray color to lips and fingernail beds
- Loss of consciousness
Second, let the person know you’re going to perform the Heimlich. Tell the choking person you want to help them. Let them know you know the Heimlich Maneuver and are going to perform it on them.

Third, wrap your arms around the person’s waist. Stand with your legs separated to best support your body, then, gently wrap both arms around their waist. Lean them forward at about 15 degrees.

Fourth, position your hands. With one hand, make a fist. Position your fist below the ribcage, but above the belly button. Then, wrap your other hand around your fist, preparing for your main “thrusting” motion.

Fifth, make a series of thrusts. To make a thrust, press hard and quick into the abdomen. Pull inward and upward as you press. It should feel like you’re trying to lift the person off the ground.
Perform five abdominal thrusts in quick succession. If the object is still not dislodged, repeat with five additional thrusts.

Sixth, perform back blows. If the object is not dislodged with the Heimlich maneuver, do back blows. Deliver five blows to the person’s back with the heel of your hand. Aim for the area between the shoulder blades.
- Press down hard, as you need to use enough force to dislodge the object. However, keep the force confined to your hands. Do not squeeze the area surrounding the person’s ribcage or abdomen.
Lastly, call emergency services. Call emergency services if the object is not dislodged. Preferably, have someone else call emergency services after the Heimlich fails the first time and you are performing another round of back blows. When an emergency service worker arrives, they can get the object dislodged. At this point, stay away from the choking person.
Where Can I Find Emergency Medical/Search/Rescue Training Program(s)?
In almost every city, there’s a person who’s well-versed in emergency medical training. If you can’t get trained or certified in your city on the numerous courses on wildmed.com, seek out your local university or community college, hospital, or community centers. If even that fails you, seek out your city officials: your firemen, your policemen, and emergency responders; they’ll point you in the right direction to find the training you need or want in your preparedness journey.
What Medicine Should I Stock Up On?
The most important criteria in selecting your medicine to store are:
(1) the medicines you need for your conditions, treatment, and overall comfort – if supply is interrupted, how much do you have?
(2) how long will what you have stored last? And have you stored it properly within the best conditions for that particular type of medicine?
(3) Over-the-counter versus prescription medications, are there any special storage concerns in addition to supply/availability?
Standard Medicines and Agents to Have in Your Medical Storage*
- Acetaminophen – pain and fever relief
- Non-steroidal anti-inflammatory drugs (NSAIDs) – brings down swelling
- Aspirin – in a heart attack, can slow down clotting of harmful (in this case) clots/platelets
- Antihistamines – for allergic reactions
- Decongestants, cough suppressants, and flu relief medicine – they help
- Antacids – stomach acidity and its management
- Antibiotic ointment -included in most checklists
- Hydrogen peroxide & rubbing alcohol – for disinfection
- Laxatives & anti-diarrhea medication – getting rid of toxins (potentially from botulism) vs fighting dehydration in the form of the “squirts”
*On storing your medicines in long-term storage, see the Freeze-Dried and Mylar Bag sections in our article on Long-Term Food Storage, A Complete Guide to Food Storage.
The Emergency First Aid Checklist
The Comprehensive Medical Supply Checklist (General)
- Syringes, cannulas, and needles – all sizes and types; including kits
- Catheters – all sizes and types; including kits
- Coils, guidewire
- Guidewires, all
- Medical tubing or hoses less than 2” diameter; including associated adaptors, connectors,
- Caps, clamps, retainers, brackets, valves, washers, vents, stopcocks, or flow sensors; and
- Peristaltic pumps with flow rates of less than 600 liters/hr for such tubing (note: does not include tubing made of butyl rubber or greater than 35% fluoropolymers)
- Endoscopic devices including laryngoscopes, laparoscopes, anascopes, proctoscopes, arthroscopes, sinuscopes, dematoscopes, ophthalmoscopes, sigmoidoscopes, otoscopes, retinoscopes, or colposcopes
- Blood pressure monitors, gauges, cuffs, aneroids, or infusors
- Monitor for glucose management
- Medical defibrillators
- Medical lavage systems
- IV sets, bags, and arm boards
- Medical penlights
- Stethoscopes
- Speculums
- Medical scissors
- Forceps
- Single-use medical procedure trays and kits
- Medical diagnostic kits, point-of-care; including EAR99 reagents
- Reflex hammers
- Blood lancets
- Ear plugs and muffs
- Otology sponges
- Ear syringes
- Ear wax removers
- Clinical swabs, applicators, specimen collectors, sponges, pads, tongue depressors, wooden spoons, cotton balls, or cotton rolls
- Antiseptic wipes for human use (including alcohol, antimicrobial, benzalkonium, betadine, iodine, and witch hazel)
- Splints
- Canes, crutches, walkers, rollators
- Patient wheelchairs, chairs, gurneys, stretchers, mats, and cots
- Patient transfer chairs, lifts, benches, boards, slides, discs, slings, and sheets
- Safety poles, rails, handles, benches, grab bars, commode aids, and shower aids
- Patient vital-sign monitoring devices
- Limb prosthesis devices
- Orthopedic supports, braces, wraps, shoes, boots, or pads
- Medical casts, padding; and casting and removal equipment
- Orthopedic traction devices and tables
- Human body positioners including pads, wedges, cradles, pillows, rests, straps, supports, and holders
- Human specimen collectors and containers (e.g., urine, blood, tissue)
- Medical bandages, gauze, dressings, tape, swabs, sponges, and burn dressings
- Surgical sutures and staples; and removal kits
- Tourniquets
- Thermometers for measuring human body temperature
- Clinical basins, bowls, baths, pans, urinals, bags, and buckets; and holding devices for such items
- Medical carafes, cups, containers, and tumblers
- Medicine cups
- Syringe aspirators
- Medical bags for medical supplies and equipment; including pre-packed bags
- Condoms
- Medical labels, labelers, stickers, forms, charts, signage, tags, cards, tape, wrist bands, documents, brochures, and graphics
- Non-electronic patient medical record file systems and organizers
- Beds: hospital beds, cribs, or bassinets; including mattresses, overlays, pillows, and bumpers
- Medical linens (e.g., blankets, sheets, pillowcases, towels, washcloths, drapes, covers)
- Chairs: exam, treatment, surgical, dental, or phlebotomy
- Stools: designed for clinical use
- Stands: IV, instrument, solution, or hamper
- Carts: medical, medical utility, medical supply, food service, or hospital laundry carts
- Tables: operating, exam, therapy, overbed, treatment, medical utility, or medical instruments
- Jars and containers designed for medical supplies and instruments less than 5 L internal volume
- Privacy screens and curtains
- Cabinets: medical supply or pharmaceutical
- Floor mats: safety, anti-fatigue, or special-purpose medical floor mats
- Hydrocollator heating units
- Warmers: bottle, gel, lotion, or blanket
- Patient heating and cooling devices: pads, packs, bottles, bags, warmers, blankets, patches, lamps, bags
- Paraffin baths
- Lights and lamps: surgical, or medical exam, magnifying
- Scales, stadiometers, rulers, sticks, tapes, protractors, volumeters, gauges, or calipers designed for human measurement
- Patient safety devices including vests, aprons, finger mitts, limb or body holders, jackets, belts, restraints, cuffs, straps, or protectors
- Human body or cadaver bags and shrouds
- Adhesive designed for human use
- Adhesive remover designed for human use
- Telemetry pouches designed for human use
- Bottles (prescription)
- Capnograph
- CPAP (continuous positive airway pressure) systems and all components
- Medical Flowmeters, oxygen & air
- Humidifiers
- Manikin, medical training, CPR
- Medical Pumps
- Ventilator, adult and tubing and accessories
- Oxygen apparatus, all
- Pulse oximeter
- Refrigerator, compartmental for morgues
- Spirometer
- Tents, pediatric, aerosol, & mist
Resources: Military Medicine PDFs
- US Army Special Forces Medical Handbook, ST 31-91B, 1 March 1982
- First Aid, U.S. Army Field Manual 4-25.11, 23 December 2002 (2.4 MB PDF)
- First Aid for Soldiers, U.S. Army Field Manual 21-11, 28 August 1989 (4.2 MB)
- Bandaging and Splinting, U.S. Army Field Manual 8-50, June 1957 (2.8 MB PDF)
- The Ship’s Medicine Chest and Medical Aid at Sea, U.S. Coast Guard, 2003 Edition (5.5 MB PDF)
- Emergency Childbirth, a joint publication of the Department of Defense and the Department of Health and Human Services, 1970
- Family Guide Emergency Health Care, a joint publication of the Department of Defense and the Department of Health and Human Services, 1971 (4 MB)
- War Psychiatry, Office of the Surgeon General, U.S. Army, 1995 (5.4 MB)
- Military Dermatology (Redacted), Office of the Surgeon General, U.S. Army, 1995 (2.8 MB)
- Unit Field Sanitation Team, U.S. Army Field Manual 4-25.12, 25 January 2002
- Hospital Corpsman, US Navy Nonresident Training Course, August 2000
- Radiation Health Protection Manual, Department of the Navy, August 2001
- Personnel Dosimetry Guidance and Dose Recording Procedures for Personnel Occupationally Exposed to Ionizing Radiation, Joint Army Pamphlet 40-18, 30 June 1995
- Handling Procedures for Equipment Contaminated with Depleted Uranium or Radioactive Commodities, US Army Pamphlet 700-48, 27 September 2002
- Disinfection and Sterilization of Dental Instruments and Materials, US Army Technical Bulletin, 31 May 1995
- Sterilizing Medical, Surgical, Dental and Veterinary Materiel, US Army Technical Bulletin, 2 May 1987
- Malaria Prevention and Control, Navy Medical Department Pocket Guide, September 2000
- Preventive Medicine, Department of the Army Pamphlet 40-11, 22 July 2005
- Preventive Medicine Services, Army Field Manual 4-02.17, 28 August 2000
- Division and Brigade Surgeon’s Handbook, Army Field Manual 4-02.21, 15 November 2000
Military Medicine | 10 First Aid Skills | Dark Angel Medical | Stop the Bleeding | Survival Medicine Handbook Essential Guide | The Top 20 Generic Molecules (Drugs) in the World | First Aid Kit Checklist | Recognizing Medical Emergencies |
Resources Continued: American Patriot Survivalist Resources on Medicine and Preparedness

The Complete First Aid Report | The First Aid Checklist | How To Build The Ultimate Survival First Aid Kit | How To Use A Butterfly Bandage for First Aid | Bugout Back Bundle | Preppers Bundle Course | How to Go Off the Grid, Step by Step | Survival Preparedness Bundle | How to Use a Tourniquet | Tactical Survival Guides | Emergency Preparedness Plan | Vehicle EDC Kit | 44 Cheap Items You Can Stockpile Now That Will Be Extremely Valuable When SHTF | How to Dress a Wound | What Should Be in a Bushcraft Kit | What is the Best Folding Knife? | 8 Survival Skills Every Prepper Needs to Know
“Always Be Ready” Max